For more information call
The Wellington Hospital: 020 7483 5589
Fortius Clinic: 0845 853 1000 The Yorkshire Clinic: 01274 621600 |
|
Adductor Injuries
Adductor injuries are very common and often reported in the news for football and rugby. The majority of adductor injuries are acute and defined as adductor sprains. Adductor injuries can also become chronic, these are difficult to treat and might seriously impact on the athletes’ performance. The adductor longus muscle plays an important role in kicking, twisting and turning in sports like football and rugby.
Acute injuries present with a sudden sharp pain on the inside of the thigh. Acute injuries occur mainly at the junction between muscle and tendon, whilst a tear between the bone and tendon is quite rare. Acute adductor injuries are partial or full thickness tears at the muscle tendon junction. Often we find a bruising on the inner side of the thigh. Treatment is non operative and consists of icing, a gentle stretching program and further functional rehab. The return to sports is usually between 3 and 6 weeks. A tear between the tendon and bone is a rare injury and has a much longer recovery, which can take between 10 and 14 weeks. This injury might sometimes require surgery with a refixation of the tendon to the bone. Prevention is important and adductor strengthening exercises during preseason can significantly reduce the risk for acute adductor injuries.
Chronic injuries can be difficult to treat and occur often at enthesis (tendon to bone attachment). The first line of treatment is a strengthening program for the adductors. Chronic adductor injuries resistant to conservative treatment can successfully be treated with an injection at the base of the tendon, a so-called pubic cleft injection. Professor Schilders was the first one to recognize the role of pubic cleft injections for chronic adductor problems. He developed, together with radiologists, an MRI imaging protocol for better diagnosis of adductor lesions. He found that in professional athletes the MRI scan was important in predicting the success of the injections. When abnormalities were found on the scan the effect usually only lasted for up to 5 weeks. In recreational athletes, however, a good result could be achieved with injections in over 75%, even when abnormalities were found on the scan. When this type of treatment is not successful, surgery is the remaining option. Adductor tenotomies, basically cutting the adductor longus tendon where it attaches to the bone, is the classic and still widely used form of surgical treatment. The results, however, were often unpredictable and there was not a consistent return to sports or to the same level of sports. Adductor injuries were often career ending injuries for the professional athlete. Ernest Schilders developed a technique where, without cutting the tendon, lengthening can be achieved with over 95% of professional athletes returning to the same level of sports. The majority of high level and professional athletes can return to sports at around 6 weeks.
A unique MRI protocol is used to investigate adductor injuries. The MRI scan will help stage the injury and decide which treatment is required.

(fig. 1 Oblique view at the level of the bladder and pubic symphysis.The white arrows point towards the zone of increased contrast uptake typical for adductor enthesopathy. The adductor enthesis is the dark area in front of the arrows.)
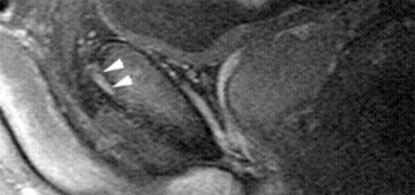
(Fig.2. MRI scan demonstrating increased signal typical for adductor enthesopathy. The dark triangle in front of the arrows is the adductor enhesis. Sagittal view through the symphysis, adductor longus and bladder.)