For more information call
The Wellington Hospital: 020 7483 5589
Fortius Clinic: 0845 853 1000 The Yorkshire Clinic: 01274 621600 |
|
Sportsmans Hernia
The sportman’s hernia, also called sports hernia or Gilmore’s groin, is a condition of the groin affecting athletes. The syndrome is often referred to as athletic pubalgia in the American literature, but this term is very confusing: it is not specific and does not differentiate between adductor pain or conditions of the rectus abdominis. With a sportsman’s hernia, we can find a tear in the front layer (external oblique fascia) of the groin canal, combined with a weakness in the muscle that forms the posterior wall of the groin canal. There is, however, no visible lump or protrusion. This condition can occur in most sports, but in Europe it is most frequent in soccer.
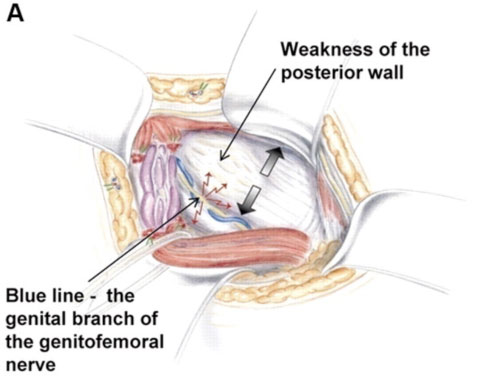
(Reprinted with the permission of Dr U Muschaweck)
Symptoms
The syndrome is characterised by chronic groin pain in athletes. The pain initially starts after sports activities, but gradually it will start to affect the athlete during sports activities. Activities such as running, accelerating, twisting, turning and kicking will be painful, as well as coughing and sneezing. The pain often radiates to the inner side of the thigh (adductor area) or to the rectus abdominis muscle. The diagnosis can easily be made solely with clinical examination, where the experienced clinician will find a dilated external inguinal ring and a weakness of the inguinal floor, or posterior wall. A ‘hernia’ as such cannot be found on clinical examination or imaging and the term ‘hernia’ is therefore a misnomer. However, experienced radiologists might be able to demonstrate a bulging of the posterior wall on ultrasound scan examination.
Treatment
Non-operative treatment of the sportsman's hernia is usually not successful. Some patients report improvement of their symptoms at rest, but the pain usually reoccurs when patients return to their sports activities.
Overall, there is a consensus that surgery is the best option to treat this condition. The surgery is performed with a minimal incision technique to repair and strengthen the torn structures. The surgery can be done as a day case or with overnight stay. Following the surgery, jogging is allowed after 7 to 10 days. Patients do core stability exercises combined with exercises to strengthen the adductors postoperatively. A return to sports is usually achieved after 4 to 6 weeks. An open repair gives more predictable outcomes than a laparoscopic repair. Laparoscopic treatment of this condition has given spectacular results, but also some spectacular failures. The reason for this being that, with a laparoscopic technique, the inguinal canal is only approached from one side, and although the posterior wall weakness can be addressed that way, neither the tear of the fascia to the external oblique or issues of nerve irritation in the canal can be addressed.