For more information call
The Wellington Hospital: 020 7483 5589
Fortius Clinic: 0845 853 1000 The Yorkshire Clinic: 01274 621600 |
|
Labral Repair
Arthroscopic repair of labral tear
Why do we repair the labrum at the London Hip Arthroscopy Centre? The labrum has an important biomechanical and nutritional function. When the function of the labrum as a stabilizer decreases, shear forces on the articular cartilage of the femoral head increase. If the surgeon were to resect the damaged labrum, these shear forces increase even more; the shear forces, however, decrease if the surgeon repairs the labrum.
The arthroscopic procedure aims to prepare the labrum and the underlying acetabular bone for primary healing of the damaged structure. Development of further degenerative changes of the hip joint (arthritis) may be prevented. Ernest Schilders uses a 2 portal technique to repair the labrum through keyhole surgery. He uses a dissection technique, which allows him to preserve as much labral tissue as possible performing the repair. An isolated tear is unusual and therefore simply repairing the labrum is not effective: it is important that the underlying cause, such as FAI or instability, is dealt with as well.
The majority of labral tears occur where the labrum attaches to the rim and to the articular cartilage. In this area, the blood supply of the labrum is very poor, making spontaneous healing unlikely. If the surgeon resects a bit of bone on the outside of the rim, creating a bleeding bed for the labrum to be refixated, the labrum can heal very well. The labrum is repaired with bioabsorbable suture anchors, usually 2 or 3.The sutures are passed around or through the labrum and tied using an arthroscopic knot tie technique, fixing the labrum against the acetabular rim.
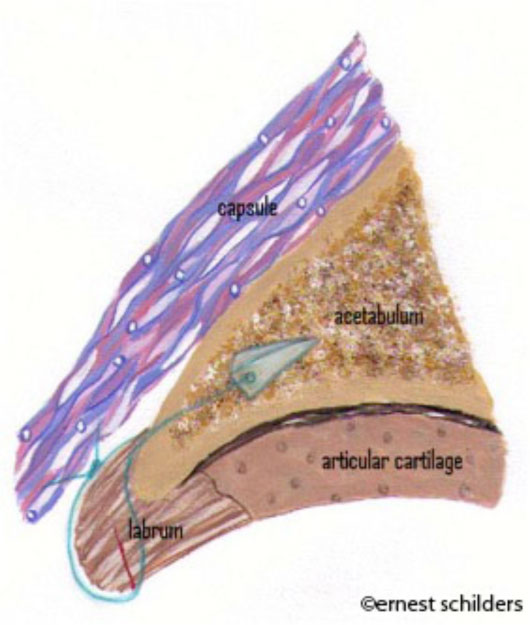
(drawing showing a labral repair. The suture anchor is placed parallel to the articular surface of the acetabulum)
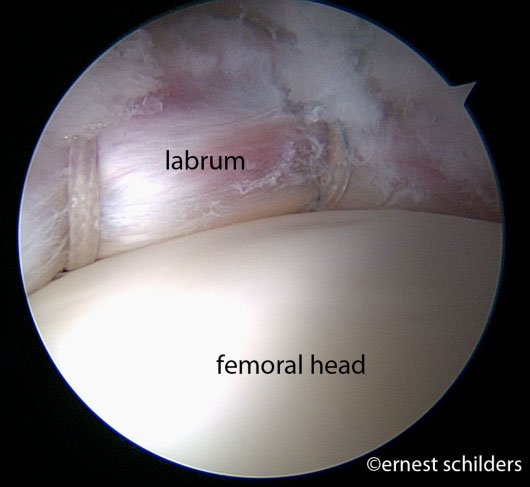
(arthroscopic picture showing a labral repair. The labrum is nicely sitting over the femoral head to work as a suction seal)
Ernest Schilders has an unparalleled experience with labral repair having performed over 400. Postoperatively, most patients use crutches, partially weightbearing for 4 weeks. Early range of motion exercises are started straight away to avoid scar tissue formation. Patients start cycling on a stationary bicycle from the first day postoperative.
Professor Ernest Schilders has produced a large study that compares the surgical results after a minimum of 2 year of follow up for this procedure. This study demonstrates significantly better outcomes for patients who had the torn labrum repaired, as opposed to those who had the labrum resected.
femoroacetabular impingement (FAI) surgery - Surgical results - Testimonials - home - Ernest Schilders profile